

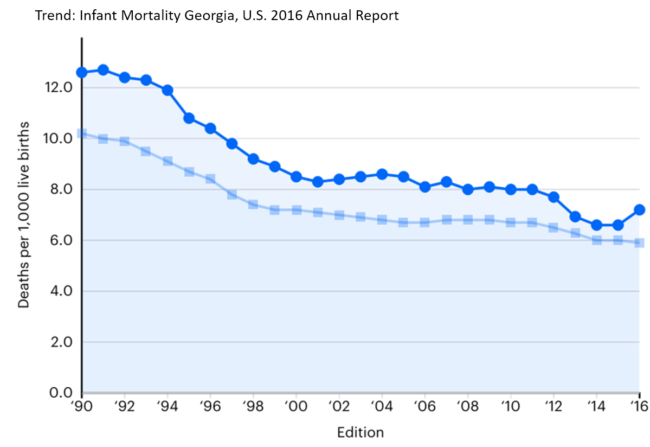
Georgia’s infant mortality rate has risen over the last few years while the national rate has flattened or declined, Department of Public Health statistics show.
In 2010, 6.3 Georgia babies for every 1,000 live births died within their first year of life. By 2015, that number had increased to 7.8.

But Lara Jacobson, director of Health Promotion at the state Department of Public Health, said Friday that preliminary data for 2016 show a decrease in the infant mortality numbers for Georgia.
Georgia was ranked 43rd among states in a recent infant mortality rating from United Health Foundation.
“We’re not where we should be,’’ Jacobson told GHN, adding. “We have put a tremendous amount of time and strategy into this.”
The main causes of infant mortality are birth defects, such as congenital heart disease; preterm births, which have recently risen in Georgia; maternal factors; and sleep-related deaths.
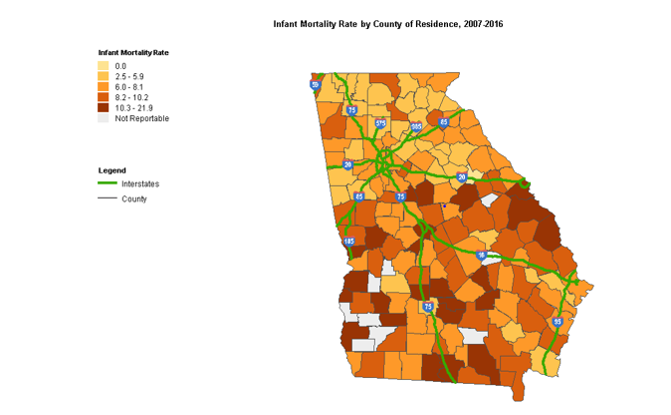
State data show that counties in the southern half of Georgia have higher infant mortality. And there’s a racial disparity as well, with babies born to black women having much greater mortality risk than those with white mothers.
Jacobson said the state has focused much of its strategy on reducing preterm births, also known as premature births.
Georgia’s preterm birth rate climbed to 11.2 percent last year, up from 10.8 percent in 2015.
“Infant mortality rates are inextricably linked to preterm birth, which often leads to low birthweight,” said Elise Blasingame, executive director of Healthy Mothers, Healthy Babies Coalition of Georgia. “The latest data available shows that of the infants who died before their first birthday, 70 percent were born low birthweight.”
Tackling the preterm birth problem involves several different strategies.
Public Health has said Georgia has seen greater use of long-acting reversible contraceptives (LARC), which can help women to better space their pregnancies. Georgia mothers who have less than one year of spacing between delivery and the next pregnancy have a 12.3 percent preterm birth rate.
Georgia Medicaid reimburses hospitals that implant LARCs. And Medicaid, which covers most births in Georgia, has stopped paying for early elective deliveries, encouraging pregnant women to go to full term.
Regional Perinatal Centers in Georgia coordinate access to optimal and appropriate maternal and infant health care. And the “Centering Pregnancy’’ initiative is a group prenatal program that combines health assessment, education and support.
Rural counties have higher infant mortality numbers, Jacobson said.
A factor in that disparity may involve longer distances to birthing hospitals, which can increase chances for preterm birth. Only 46 of Georgia’s 159 counties have labor and delivery units, with about 75 hospitals in the state routinely delivering babies, according to the Georgia OB/GYN Society.
“There is a higher preterm birth rate overall in rural counties,’’ Jacobson said recently.
Other factors that help reduce the mortality risk include breastfeeding, the WIC program’s nutrition help, and Safe to Sleep programs, Jacobson said.

In the Safe to Sleep program, parents and caregivers are urged to follow these guidelines:
Alone – babies should sleep alone in their own sleep space, close to but separate from their caregiver.
Back – babies should be placed on their backs to sleep. Every nap. Every sleep. Every time.
Crib – babies should sleep in a crib or bassinet with a firm, flat surface with no extra things such as crib bumpers, blankets or toys.